






Fixing a Botched Surgery
Dr. Arun C. Gulani is a world destination for patients who have had “Botched” surgeries elsewhere as in complications of Cataract surgery, Multifocal lens implants, Lasik complications, Keratoconus, Radial Keratotomy surgical complications etc.




He not only provides hope but fights for each patient’s vision to his best ability as is noted by patients who seek him from all over the globe. Noted eye surgeons from all over the country and world regularly refer their complications to Dr. Gulani with full confidence that he has the track record, surgical skills and integrity in only doing what is right for the patient in not only salvaging their complications but in most cases bringing their vision to 20/20.
Over three decades, as a Master surgeon, Dr. Gulani has developed a systematic approach with unlimited technology and techniques; KLEAR™, which includes all forms of surgeries including Corneal (Kerato), Lens Implants/Cataract/ICL (Lenticulo), Lasik/PRK/LenZoPlastique/Intacs/CXL (Refractive). By using KLEAR™ and GPS™, Dr. Gulani has successfully addressed not only normal candidates but those with complex and Botched surgeries in many cases to 20/20 vision outcomes.
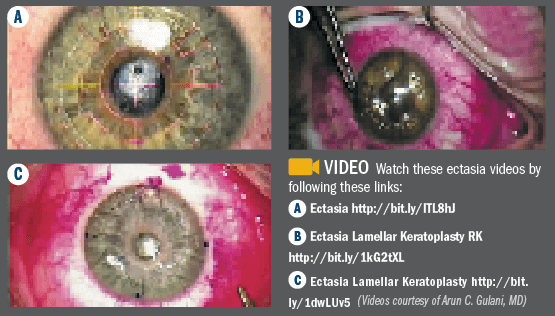
In cases of ectasia, we would first suggest that we not even use that word. Using names like “ectasia” causes trepidation and knee-jerk reactions among surgeons and despair among patients.
In addition to the natural cause of keratoconus, ectasia can arise from LASIK, automated lamellar keratoplasty, radial keratotomy, trauma, etc. The cause, technology that caused it, name of the surgeon, or state or country where it was done is immaterial when we approach ectasia in a holistic vision rehabilitative mode.
The backbone behind technique selection and plan formation for any patient—including those with ectasia—is the 5S system classification of Sight, Scar, Shape, Strength, and Sit.
The 5S system can be used to melt down the complexity of this condition into basics. Take the worst and most feared complication of visual corrective surgery and reverse it by using the principles of refractive surgery as an art to return the patient not only to usable vision, but also to best vision potential (BVP).
To Dr. Gulani’s fellows, we like to introduce the 5S system as a “coin sorter.” Throw any surgical complication into it and watch it break the complex and scary giant into manageable components. Then, like Lego pieces, use this to plan surgery toward BVP (see “Vision á la carte: Designing Vision,” Ophthalmology Times, Sept. 15, 2013, Page 31; “Multifocal IOL nightmare: Reversed to 20/20,” Ophthalmology Times, Oct. 1 2013, page 18),.
The most common cases of ectasia usually have the following 5S factors affected: Sight (vision potential), Strength (decreased thickness), and Shape (irregular astigmatism/myopia).
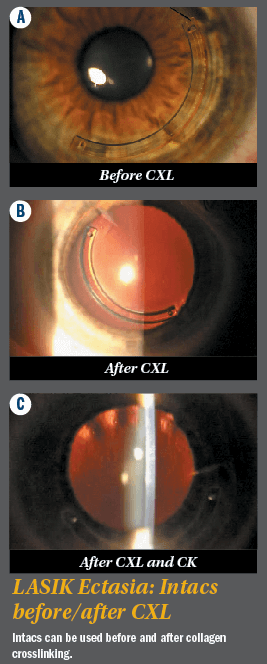
Looking at the most common case scenario—post-LASIK ectasia—approaching the affected factors can be undertaken using intrastromal corneal ring segments (Intacs, Addition Technology) in uniquely designed configurations to induce directional optical manipulations with ring segments single and paired, superficial and deep, thick and thin segments, and intended axis entry.
By using directional entry into the cornea, for example, the intrastromal corneal ring segments can be uniquely arranged not only to flatten the cornea (decreasing keratometry and myopia), but also to correct astigmatism (axis oriented entry of the intrastromal corneal ring segments) and correct the strength (although this will not add tissue, it will add strength, like braces)—resulting in improved configuration, which translates to improved sight.
Once this stability is achieved, residual astigmatism (the most common residual refractive error following these cases) can be addressed by laser PRK—since we know that removal of astigmatism with the excimer laser utilizes the least amount of tissue ablation and also the already placed intrastromal corneal ring segments, like braces, will provide supportive strength to tissue removal.
This can further be followed, in the near future, by collagen crosslinking (CXL) to make the achieved outcome permanent.
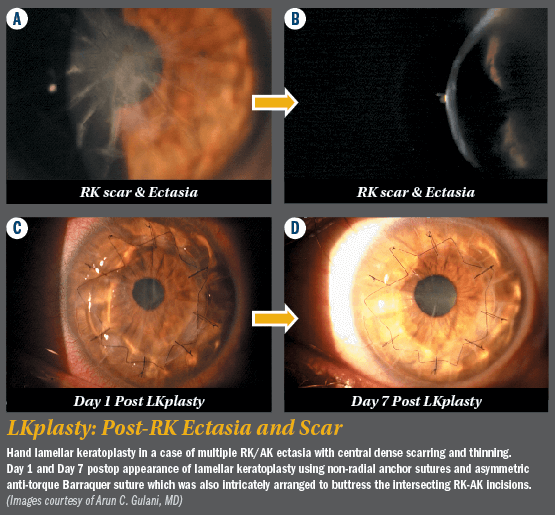
Now, take a scenario in which the most commonly affected three S’s of ectasia are present with the additional fourth S of Scar.
In cases of corneal ectasia with scar, in addition to the involvement of strength and shape, lamellar keratoplasty can be used, such that the tissue lamella that is replaced adds strength by adding thickness, removes the scar, and also aids with shape by decreasing the keratometry by flattening, thus decreasing ectatic myopia. In most cases, the astigmatism will be either neutral or slightly decreased.
Having corrected these S factors, 6 months after suture removal and stability, excimer laser in PRK mode could be used to correct the refractive error back to emmetropia, and in the near future, once again, CXL to make the procedure permanent.
Additionally, intraocular surgery can be undertaken to manipulate the eye optically either before or after corneal stabilization using phakic or pseudophakic lens implants.
For example, if the patient is at the age of cataracts, a surgeon can actually utilize toric IOLs to correct the patient’s refractive error and induce a level of myopia for future laser flattening (decreasing keratometry) and smoothing of the cornea.
Laser PRK in the myopic mode should be used as the final wand in re-establishing emmetropia and final contour to vision.
Plus, all steps prior to this would optically arrange or manipulate the eye toward a stable myopic astigmatism outcome to use the cornea as what we call a “laser vision rehabilitative platform” (given its easy accessibility).
CXL can be used in all such cases as a final “permanizing” procedure, as opposed to using it as a first step in “cementing” the ectasia. We use the analogy of a bent, scoliotic spine here. Rather than cementing (akin to CXL) the bent, scoliotic spine so it will not bend anymore, we would rather first correct that curvature to best functional use (akin to vision and anatomy), using whatever means (akin to ectasia, intrastromal corneal ring segments/lamellar Kplasty/CK), and only then proceed with cementing or permanizing the outcome (akin to CXL).
The point is to take the patient with ectasia closer—with every step—to the end zone. Maintain the principles of Corneoplastique, keeping all surgical steps brief, elegant, visually promising, least interventional, with all standard surgeries (like penetrating keratoplasty) acting as back-up, and return patients to the very goal they began this journey with—BVP—restoring not only vision, but faith and hope.