






CORNEAL SCAR Treatment Repair Vision to 20/20
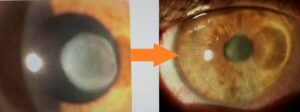 The worst insult from a complication of any cornea based surgery including Lasik/Contact lens infection/etc is a corneal scar. Corneal scar can blind people.
The worst insult from a complication of any cornea based surgery including Lasik/Contact lens infection/etc is a corneal scar. Corneal scar can blind people.
The traditional thinking for a corneal scar has always been to get rid of it and the tissue that contains it ie. Corneal transplant. When looking at a corneal scar, our inherent mindset is : “There is the culprit. Let’s eradicate it.” Numerous diagnostic technologies are then deployed to “Understand the scar and its obviously criminal impact on Vision”.
Then—in their minds—many ophthalmologists go through an elegant and complicated thought process to determine whether to choose laser PTK (an optically incorrect surgery), diamond burr application (a barbaric procedure on an elegant visual organ), or a corneal transplant (a relatively interventional procedure that should be the last resort, very much like having to finally open the entire abdomen to get to the gall bladder) as the correct treatment for this corneal scar.
Let us assume also a mindset that thinking about performing a corneal graft (Penetrating keratoplasty : PKP) is akin to giving up, losing the battle, or not even venturing to design vision in our patient’s best interests. Unless there is a through-and-through corneal pathology/perforation from whatever cause (trauma, infection, surgical complications, degeneration, etc.), a penetrating corneal transplant should be the last resort of corneal rehabilitative techniques.
As I have said before, PKP can be compared to opening the entire abdomen as opposed to elegantly approaching individual structures with the least interventional attitude. It does not matter how you do the penetrating transplant, i.e., femtolaser, microkeratome, or even a kitchen knife; what matters is how you put it back together (since shape translates to refraction and refraction translates to vision) and hand stitching of the transplant leads to astigmatism and vision distortion, not to mention rejection issues including heightened possibility of glaucoma, cataracts and lifetime danger of the graft coming apart with trauma.
Corneal Scar Treatment
Using our 5S system, most corneas that are structurally abnormal, unstable, or compromised should undergo corneal scar treatment with an elegant thought process using Corneoplastique™ principles (brief, topical, aesthetically pleasing, visually promising) to rehabilitate that cornea with the least interventional approach for that patient and present it as a vision rehabilitative platform (VRP).
What I suggest instead is to look at the corneal scar and ask yourself, “How can I use this or modify this to help the patient see better with the least intervention” and “Is it necessary to remove this and at what cost?”
This is the paradigm shift in thinking and the future of molding corneal scars to our advantage (by whatever surgical means and combinations) to therewith improve refraction and hence the vision.
Anterior corneal scars affect vision directly by blocking the optical pathway, and indirectly, by altering the shape, and hence the refractive status. Using Corneoplastique principles, we can use these very factors and reverse them to our advantage.
In the Gulani 5S algorithm, you can see the impact of the corneal scar on vision and determine the patterned approach of corneal scar treatment, rehabilitation and laser or direct laser, and straight reshaping to vision. The refraction is the mainstay of the corneal scar algorithm, where vision better than 20/30 suggests straight laser PRK; while less than 20/40, following a hard contact lens trial, can determine staged laser in two stages or a scar peel, followed by myopic ablation.
For the sake of simplicity, I have divided corneal scars into ‘on-cornea’ scars, which are above the Bowman’s membrane and lead to a camouflaged topography and misleading refractive error and “In-cornea’ scars, which actually become part of the cornea and are directly responsible for the topography, and have a direct correlate to the refractive error. Hence, these can be lasered through.
Instead of laser PTK, which chases the scar and distorts the shape (costing us in vision), why not reshape the cornea and take it straight to vision (in many cases, despite a residual scar)?
Understanding On-cornea and In-cornea scars
On-cornea scars can be peeled off right under the laser using the cornea as what I call a “resistance-guided platform” which is comprised of pulling on the scar, making sure you remove it completely, in one piece, using the rest of the cornea as your resistance platform. This is followed by Refractive PRK (always with mitomycin C application)as single stage or Myopic PRK to be followed by stage two for refractive PRK to emmetropia.
Deeper on-cornea scars can also be peeled off using patience and a resistance-guided technique as well to gently peel them off of the rest of the cornea. Once again, try to maintain the entire piece as a single removal technique. Once it clears the visual axis, you can proceed with refractive laser PRK ablation, followed again by the application of mitomycin C. This corneal scar treatment can result in complete central clarity, to an excellent outcome.
In-cornea scars can be Lasered directly in the ASA/PRK mode, shaping the cornea, and indirectly removing the scar, straight to a visual outcome. In cases of on-cornea scars, the scar can be gently peeled off, maintaining all the principles we discussed about using the corneal platform as a resistance guided technique in lifting the entire scar gently, in full completion, off the remaining cornea. This is followed by laser PRK with mitomycin C and a bandage contact lens, to reach tremendous visual outcomes (Single or Two-Staged).
Thus Corneal scar treatment can be in the form a vision corrective surgery with corneal transplant as a back up in helping people see despite the scars and in many cases 20/20